‘WRECKREATIONAL’ DRUGS
“Recreational” drug use is a misnomer – put a ‘w’ on the front and you’d be closer to the truth
Former Wellington coroner Garry Evans
 As commercialisation increases in legalized states, false advertising of marijuana products as being “natural” and “healthier than alcohol and tobacco” have greatly decreased the perceived risk of harm related to marijuana use. The main psychoactive ingredient in marijuana, THC, has now been observed to cause many different types of mental and physiological health problems— especially in children and youth.
As commercialisation increases in legalized states, false advertising of marijuana products as being “natural” and “healthier than alcohol and tobacco” have greatly decreased the perceived risk of harm related to marijuana use. The main psychoactive ingredient in marijuana, THC, has now been observed to cause many different types of mental and physiological health problems— especially in children and youth.
While public opinion has been moving toward the legalisation of marijuana, science and medicine has been moving toward broad agreement on marijuana’s harms and dangers!
According to virtually every scientific review, including a 2016 World Health Organisation (WHO) report and a 2017 National Academy of Sciences study, marijuana is addictive and harmful – despite rhetoric from the marijuana industry. According to the WHO, regular cannabis users can develop dependence on the drug. The risk may be around 1 in 10 among those who ever use cannabis, 1 in 6 among adolescent users, and 1 in 3 among daily users. Withdrawal syndrome is well documented in cannabis dependence.
There are currently in circulation over 26,000 evidence-based research articles, papers and other literature covering the inherent physical, psychological, environmental, social, familial and community harms of cannabis. This includes the detailed and renowned 2016 cannabis report from the World Health Organisation.
“Why do nations schedule drugs? …… Nations schedule psychoactive drugs because we revere this three-pound organ (of our brain) differently than any other part of our body. It is the repository of our humanity. It is the place that enables us to write poetry and to do theatre, to conjure up calculus and send rockets to Pluto three billion miles away, and to create iPhones and 3D computer printing. And that is the magnificence of the human brain. Drugs can influence [the brain] adversely. So, this is not a war on drugs – this is a defence of our brains, the ultimate source of humanity.”
Dr Bertha Madras, Professor of Addiction Psychiatry at Harvard Medical School
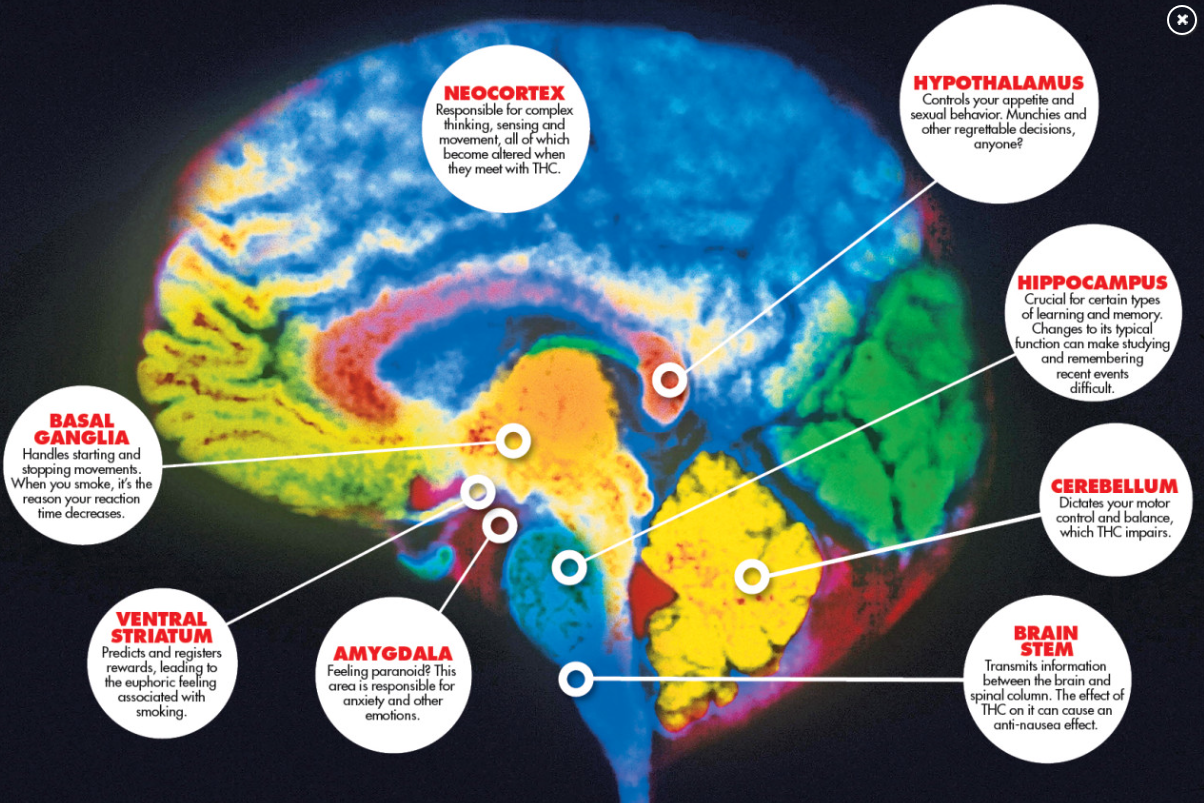
HOW DOES MARIJUANA AFFECT THE BRAIN?
Source: NATIONAL INSTITUTE ON DRUG ABUSE (June 2018)
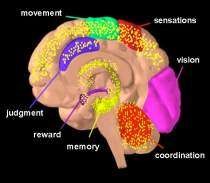
Marijuana has both short-and long-term effects on the brain. THC acts on numerous areas in the brain (in yellow).
Image by NIDA
SHORT-TERM EFFECTS
When a person smokes marijuana, THC quickly passes from the lungs into the bloodstream. The blood carries the chemical to the brain and other organs throughout the body. The body absorbs THC more slowly when the person eats or drinks it. In that case, they generally feel the effects after 30 minutes to 1 hour.
THC acts on specific brain cell receptors that ordinarily react to natural THC-like chemicals. These natural chemicals play a role in normal brain development and function.
Marijuana over-activates parts of the brain that contain the highest number of these receptors. This causes the “high” that people feel. Other effects include:
- altered senses (for example, seeing brighter colours)
- altered sense of time
- changes in mood
- impaired body movement
- difficulty with thinking and problem-solving
- impaired memory
- hallucinations (when taken in high doses)
- delusions (when taken in high doses)
- psychosis (when taken in high doses)
LONG-TERM EFFECTS
Marijuana also affects brain development. When people begin using marijuana as teenagers, the drug may impair thinking, memory, and learning functions and affect how the brain builds connections between the areas necessary for these functions. Researchers are still studying how long marijuana’s effects last and whether some changes may be permanent.
For example, a study from New Zealand conducted in part by researchers at Duke University showed that people who started smoking marijuana heavily in their teens and had an ongoing marijuana use disorder lost an average of 8 IQ points between ages 13 and 38. The lost mental abilities didn’t fully return in those who quit marijuana as adults. Those who started smoking marijuana as adults didn’t show notable IQ declines.
In another recent study on twins, those who used marijuana showed a significant decline in general knowledge and in verbal ability (equivalent to 4 IQ points) between the preteen years and early adulthood, but no predictable difference was found between twins when one used marijuana and the other didn’t. This suggests that the IQ decline in marijuana users may be caused by something other than marijuana, such as shared familial factors (e.g., genetics, family environment). NIDA’s Adolescent Brain Cognitive Development (ABCD) study, a major longitudinal study, is tracking a large sample of young Americans from late childhood to early adulthood to help clarify how and to what extent marijuana and other substances, alone and in combination, affect adolescent brain development.
WHAT ARE THE OTHER HEALTH EFFECTS OF MARIJUANA?
Marijuana use may have a wide range of effects, both physical and mental.
 Physical Effects
Physical Effects
- Breathing problems. Marijuana smoke irritates the lungs, and people who smoke marijuana frequently can have the same breathing problems as those who smoke tobacco. These problems include daily cough and phlegm, more frequent lung illness, and a higher risk of lung infections. Researchers so far haven’t found a higher risk for lung cancer in people who smoke marijuana.
- Increased heart rate. Marijuana raises heart rate for up to 3 hours after smoking. This effect may increase the chance of heart attack. Older people and those with heart problems may be at higher risk.
- Problems with child development during and after pregnancy. One study found that about 20% of pregnant women 24-years-old and younger screened positive for marijuana. However, this study also found that women were about twice as likely to screen positive for marijuana use via a drug test than they state in self-reported measures. This suggests that self-reported rates of marijuana use in pregnant females is not an accurate measure of marijuana use and may be underreporting their use. Additionally, in one study of dispensaries, nonmedical personnel at marijuana dispensaries were recommending marijuana to pregnant women for nausea, but medical experts warn against it. This concerns medical experts because marijuana use during pregnancy is linked to lower birth weight and increased risk of both brain and behavioral problems in babies. If a pregnant woman uses marijuana, the drug may affect certain developing parts of the fetus’s brain. Children exposed to marijuana in the womb have an increased risk of problems with attention, memory, and problem-solving compared to unexposed children. Some research also suggests that moderate amounts of THC are excreted into the breast milk of nursing mothers. With regular use, THC can reach amounts in breast milk that could affect the baby’s developing brain. More research is needed. Read the Marijuana Research Report for more information about marijuana and pregnancy.
- Intense Nausea and Vomiting. Regular, long-term marijuana use can lead to some people to develop Cannabinoid Hyperemesis Syndrome. This causes users to experience regular cycles of severe nausea, vomiting, and dehydration, sometimes requiring emergency medical attention.
Mental Effects
Long-term marijuana use has been linked to mental illness in some people, such as:
- temporary hallucinations
- temporary paranoia
- worsening symptoms in patients with schizophrenia—a severe mental disorder with symptoms such as hallucinations, paranoia, and disorganized thinking
Marijuana use has also been linked to other mental health problems, such as depression, anxiety, and suicidal thoughts among teens. However, study findings have been mixed.
RESPIRATORY
 Cannabis is harmful to the lungs, but in a different way to tobacco, causing significant respiratory symptoms such as bronchitis with evidence to suggest it can result in destructive lung disease –sometimes referred to as ‘bong lung’ – in heavy cannabis users. These are the key findings from a review of research on the effects of smoking cannabis on the lungs undertaken by respiratory specialists, Professor Bob Hancox, from the University of Otago’s Department of Preventive and Social Medicine and Dr Kathryn Gracie, from Waikato Hospital’s Respiratory Department. “The potential for adverse effects on respiratory health from smoking cannabis has had much less attention than the social and mental health effects. We believe policies around the liberalisation of cannabis should consider the potential impacts on the lungs… there is sufficient evidence that cannabis causes respiratory symptoms and has the potential to damage both the airways and the lungs… Many people smoke both cannabis and tobacco and are likely to get the worst of both substances.”
Cannabis is harmful to the lungs, but in a different way to tobacco, causing significant respiratory symptoms such as bronchitis with evidence to suggest it can result in destructive lung disease –sometimes referred to as ‘bong lung’ – in heavy cannabis users. These are the key findings from a review of research on the effects of smoking cannabis on the lungs undertaken by respiratory specialists, Professor Bob Hancox, from the University of Otago’s Department of Preventive and Social Medicine and Dr Kathryn Gracie, from Waikato Hospital’s Respiratory Department. “The potential for adverse effects on respiratory health from smoking cannabis has had much less attention than the social and mental health effects. We believe policies around the liberalisation of cannabis should consider the potential impacts on the lungs… there is sufficient evidence that cannabis causes respiratory symptoms and has the potential to damage both the airways and the lungs… Many people smoke both cannabis and tobacco and are likely to get the worst of both substances.”
In 2007, NZ scientists studied 339 marijuana and cigarette smokers, and determined that smoking ONE joint of marijuana was comparable to the effects on airflow obstruction of between 2.5 – 5 tobacco cigarettes, “Adverse effects [of marijuana] on lung function is of major public health significance,” the study authors warned.
A 2007 review of 34 studies on marijuana use and lung function found short-term exposure to marijuana is associated with bronchodilation, and long-term marijuana smoking is associated with increased respiratory symptoms suggestive of obstructive lung disease.
PSYCHOSIS
“The link between cannabis and psychosis is quite clear now; it wasn’t 10 years ago.”
Professor Colin Blakemore, chief of the Medical Research Council (UK) (2007)
A study published in the American Journal of Psychiatry further links the use of marijuana with the onset of severe mental illness such as psychosis and schizophrenia. The study followed over 7,600 individuals for a mean of 84 months. Among these, the cumulative risk for progression to schizophrenia was 11.3%. The risk for onset of mental illness was highest among marijuana users and lowest for alcohol abusers.
In 2011, Australian researchers did a large systematic review (meta-analysis) using 83 studies for the Archives of General Psychiatry. They said; “The results of meta-analysis provide evidence for a relationship between cannabis use and earlier onset of psychotic illness, and they support the hypothesis that cannabis use plays a causal role in the development of psychosis in some patients. The results suggest the need for renewed warnings about the potentially harmful effects of cannabis.”
LUNG CANCER
Nine scientists from the Medical Research Institute of New Zealand examined 79 cases of lung cancer and 324 control patients and concluded: “long-term cannabis use increases the risk of lung cancer in young adults.”
According to the British Lung Foundation, “smoking three or four marijuana joints is as bad for your lungs as smoking twenty tobacco cigarettes.” THC, the primary psychoactive ingredient of cannabis, decreases the function of immune system cells that help protect the lungs from infection.
HEART HEALTH
Jan 2020
Compared with prescription drugs, the health consequences of using marijuana are not nearly as well studied. But converging evidence suggests that the drug may be harmful for the heart, according to a review article in JACC: Journal of the American College of Cardiology. “Marijuana is becoming increasingly potent, and smoking marijuana carries many of the same cardiovascular health hazards as smoking tobacco.”
People who use marijuana may be three times more likely to die from high blood pressure than non-users of the drug, a new study finds. The researchers say that their findings indicate that marijuana use is a greater risk factor for poor cardiovascular health than cigarette smoking.
Marijuana ‘may be worse than cigarettes for cardiovascular health’ – Medical News Today, Aug 2017
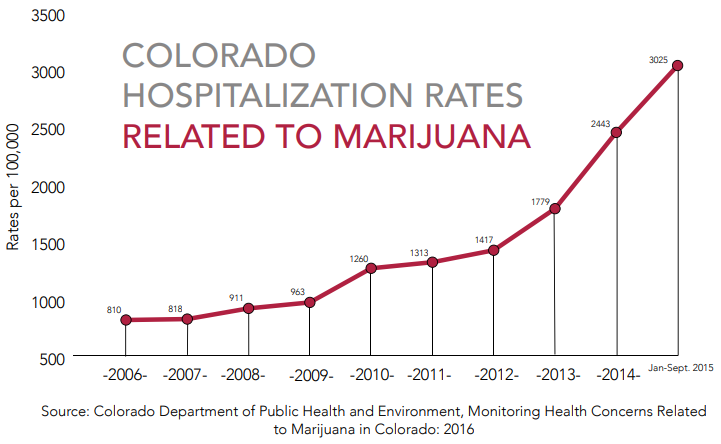
HOSPITALISATION
Colorado – The yearly rate of emergency department visits related to marijuana increased 52% after the legalisation of recreational marijuana. (2012 compared to 2016). The yearly rate of marijuana-related hospitalisations increased 148%. A recent study conducted in Colorado finds that following recreational marijuana commercialisation in 2013, marijuana-detection rates significantly increased among traumatic injury patients in Colorado hospitals (Chung, et al., 2019).
The yearly number of emergency department visits related to marijuana increased 54%, and a 101% increase in hospitalisations. The percent of suicide incidents in which toxicology results were positive for marijuana has increased from 14% in 2013 to 23% in 2017 (Rocky Mountain High Intensity Drug Trafficking Area 2019)
In Colorado, calls to poison control centers have risen 210% between the four-year averages before and after recreational legalisation.
Washington has seen a 70% increase in calls between the three-year averages before and after legalisation. The Washington Poison Control reported 378 cases of toxic exposure to marijuana in 2017. A study conducted in Washington State found that the rate of pediatric exposures to marijuana (children aged 9 or under) was 2.3 times higher following retail sales than it was before legalization (Thomas, et al., 2019).
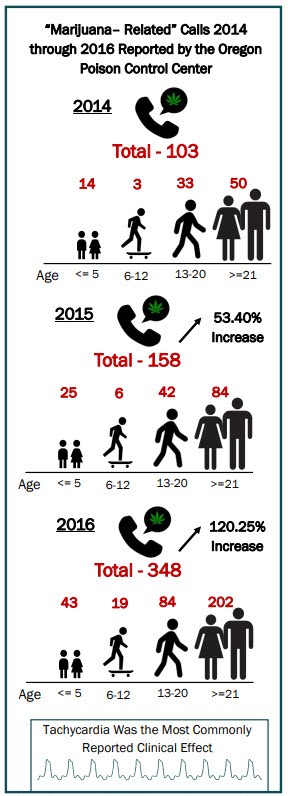
In Oregon, for children 5 years or younger, the number rose by 271% from 14 cases in 2014 to 52 cases in 2017 (Oregon Poison Center, 2018).

Central Oregon hospitals saw a nearly 2,000% increase in emergency room visits due to marijuana poisoning, with 434 marijuana-related emergency visits in January 2016 alone, compared to a maximum of 32 visits per month prior to legalization.
The increase in marijuana-related emergency room visits in Oregon includes a growing number of Butane Hash Oil (BHO) burn victims. BHO is a marijuana concentrate that yields a THC potency of 70–99% and is highly lucrative. Production involves forcing raw marijuana and butane into a reaction chamber, which creates a highly combustible liquid that easily explodes when introduced to an ignition source.(Think P-Lab!)
According to publicly available information from the Oregon Poison Control Center, calls regarding cannabis exposure grew most dramatically in the 21 years and older population – representing 60% of all calls.
2018: KIWI CHILDREN HOSPITALISED FOR MARIJUANA POISONING
Here in New Zealand, Ministry of Health figures gained under the Official Information Act in November 2018 show that 73 children have been hospitalised in the past five years either for poisoning or for mental and behavioural disorders due to the use of cannabis. This is over four times the number of hospitalisations compared to synthetic cannabis for the same age group. For all ages, more than 2,200 have been hospitalised for cannabis alone.
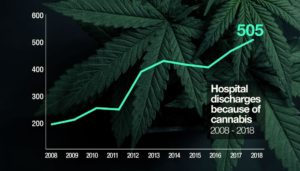
Statistics, collected by the Ministry of Health, show that in 2008 only 192 people were released from hospital with a primary cannabis diagnosis. However, by 2018, this had increased to 505.
CANNABIS AS A GATEWAY DRUG
“Consistent evidence has shown that cannabis use almost always precedes the use of other illicit drugs, including cocaine, methamphetamine, hallucinogens (including LSD and ecstasy), illegally obtained prescription drugs, and opiates, such as heroin or morphine. Cannabis users are significantly more likely than non‐users to use other illicit drugs, and more frequent use of cannabis and younger age of initiation to the drug strengthen this relationship, even after controlling for potential confounding variables and studying twins. This use pattern is strongest in adolescents and declines with age, possibly because of increased social maturity on the ability to resist illicit drug use.”
UNODC (United Nations Office on Drugs and Crime): Cannabis A Short Review (2012)
Direct associations have been made between the frequency of marijuana use and higher THC potency with the development of mental health issues (psychosis, depression, anxiety, suicidality, reshaping of brain matter, and addiction). Links to lung damage and serious cardiovascular problems have also been found (hypertension, myocardial infarction, cardiomyopathy, arrhythmias, stroke, and cardiac arrest). Marijuana use during pregnancy has also been shown to negatively affect the cognitive development of children by increasing their risk of hyperactivity, impulsivity, and inability to focus.
Chronic adolescent marijuana use has been correlated with cognitive impairment and a decreased ability to do well in work or school.
Marijuana has a variety of other interactions with mental health. While the popular view holds that marijuana is not addictive, brain scans of marijuana users show changes in the structure of the brain’s reward center to be consistent with addiction. Heavy users have also been clearly observed to have withdrawal symptoms. In Colorado, marijuana is the second drug most often implicated in addiction treatment admissions, after alcohol.
Furthermore, a number of studies have identified marijuana’s role in the pathway to other substance abuse. For example, a groundbreaking study of over 30,000 Americans showed that participants who reported marijuana use in the previous year were 2.6 times more likely to abuse prescription opioids.
Colorado toxicology reports show the percentage of adolescent suicide victims testing positive for marijuana has increased. This is not terribly surprising, as daily marijuana use among youth who begin before the age of 17 significantly increases the risk of suicide attempts.
CANNABIS WITHDRAWAL – “SCROMITING”
Cannabis withdrawal was included in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). According to researchers in San Diego, “Long-term and very heavy marijuana use may cause severe stomach pain and vomiting in a very small percentage of users. Cannabinoid Hyperemesis Syndrome (CHS) causes symptoms ranging from severe stomach pain, nausea, vomiting and the impulse to take hot showers… the condition has become so common, ER staff have coined a new term that helps identify it: “scromiting,” for “screaming” and “vomiting.”
A review and meta-analysis with over 23,000 participants conducted by researchers from Queen’s University in Ontario and the University of Calgary and published in the JAMA Network Open in March 2020, found that 47% of regular marijuana users experience symptoms of Cannabis Withdrawal Syndrome (CWS) when they cease use of the drug. The study’s authors said that because “many CWS criteria are depression or anxiety symptoms, regular users may seek cannabis to obtain short-term symptom relief, unaware that this use could perpetuate a longer-term withdrawal problem.” Also, a review of recent research published in the journal JAMA Psychiatry, states that in the states that have legalised marijuana, prices for the drug have decreased, while use and dependence has increased among adults. Furthermore, the review states that the risk of dependence has risen from around 9% in the early 1990s, to nearly 30% today.
In a case report published in the British Medical Journal Case Reports, researchers said a 27-year-old, from Minnesota, was brought to the Mayo Clinic six times over the course of a year complaining of nausea, vomiting and abdominal pain. The cannabinoid hyperemesis syndrome (CHS) occurs in heavy marijuana users, those who smoke at least 20 times a month, who have recurrent and severe bouts of nausea, vomiting and abdominal pain. The number of people affected by CHS is unclear, although its prevalence could be in the millions.
A 2015 study found that the incidence of cyclic vomiting doubled in Colorado after weed was legalized, as well as incidence of CHS rising in other states where the drug is legal. The first study to report on the phenomenon was led by Mount Barker Hospital in Australia, where researchers realized patients who had repeat attacks of vomiting had one thing in common: chronic cannabis use.
Source: https://nypost.com/2018/05/22/all-the-ways-marijuana-can-hurt-your-health/
A psychiatrist’s perspective on the harms of recreational marijuana legalisation